
The Pressure at the Base of My Skull
I was at the conference room table trying to read a legal framework and I couldn’t get past the same section. I’d read it, lose it, go back and read it again. The whole time, the ice pick was jabbing at the base of my skull. It was pain. It was also brain fog.
It didn't stop. It was there when I sat down on the train in the morning. Still there when I reached into my backpack for the prescription NSAIDs. Two pills. Hoping they’d take the edge off.
They didn’t.
Underneath the ice pick was a deeper pressure that never lifted. On the worst days, the pain expanded, spreading across the top and sides of my head in pulsating waves. I told my doctors it felt as if people were inside my head, knocking to get out. Like a beam driven through above my right eye and out the back of my skull.
They wrote down migraines. Sometimes headaches. Later occipital neuralgia. The question of whether something structural was causing the pressure at the base of my skull never made it into the chart.
Have you ever left an appointment wondering if you said it wrong? I did. That question stayed with me for years.
What It Took From Me
These episodes kept increasing in frequency. Three quarters of every month. When they hit, I had to lay down and not move. Any movement and I would throw up. They stole entire days from me, sometimes more than one in a row.
I sat in my primary care provider’s office and told her I couldn’t go on like this. The specialists kept calling it facial migraines. I told her I didn’t believe them anymore. That my daughter had asked me for a tissue and I had fallen apart. I had nothing left.
She prescribed an antidepressant and referred me to a rheumatologist. Another specialist to go see and another months-long wait. Another delay while the pain kept getting worse.
What the Commute Looked Like
On the way in, I worked through options. Spa music first. Then nature sounds, waterfalls and birds. The Tibetan sound bowls and tonal music. None of it touched the ice pick. I eventually landed on podcasts. Something to follow that didn't require me to look down at a screen. It was the only thing that made the fifty minutes manageable.
The ride home was different. By then there was nothing left. I'd sit in my seat and stare out the window. The ice pick had been there since morning. It would still be there when I got off. I watched the stops go by.
What They Tried
After prescription NSAIDs and Botox injections didn’t work, they sent me to pain management. Twenty trigger point injections across my neck, shoulders, and upper back. They didn’t help. And every time I went back, I would beg them to put the needle in the back of my head, right where the ice pick was.
“Oh no,” they’d say. “That’s only for neurology. We don’t touch the head.”
Pain management wouldn’t treat the part of my body that hurt the most. I had a neurology appointment scheduled, but it was nine months out.
Before I made it there, I went to the emergency room. I started having involuntary movements. They did a CT scan and sent me home. Good news, they said. The scan came back normal, see your neurologist. Normal scan. Still in pain. Still no answer.
I called the neurologist’s office to tell them about the ER visit and the new symptoms. They didn’t move my appointment up.
When I finally got in, the neurologist gave it a new name: occipital neuralgia. Then he gave me thirty trigger point injections in a single appointment, throughout my head and the back of my neck.
They didn’t work either.
I couldn’t take it anymore. The pain was constant and wearing me down to someone I didn’t want to be. The next suggestion was a C2 occipital nerve ablation, a procedure that would burn the nerve to stop the pain signals.
What Stopped Me
I was desperate enough to consider it. Twenty years of compliance and audit work had trained me to look for root causes. Burning a nerve was not getting to the root cause. No one had explained what was actually causing the pain. I needed to know why.
So I went home and started researching on my own. One night on my laptop, I found an article describing patients with symptoms like mine: pain at the skull base, dizziness, facial tension. The author described advanced imaging that could reveal structural causes that standard tests were missing.
It was the first time someone was looking for why.
What Was Underneath It All
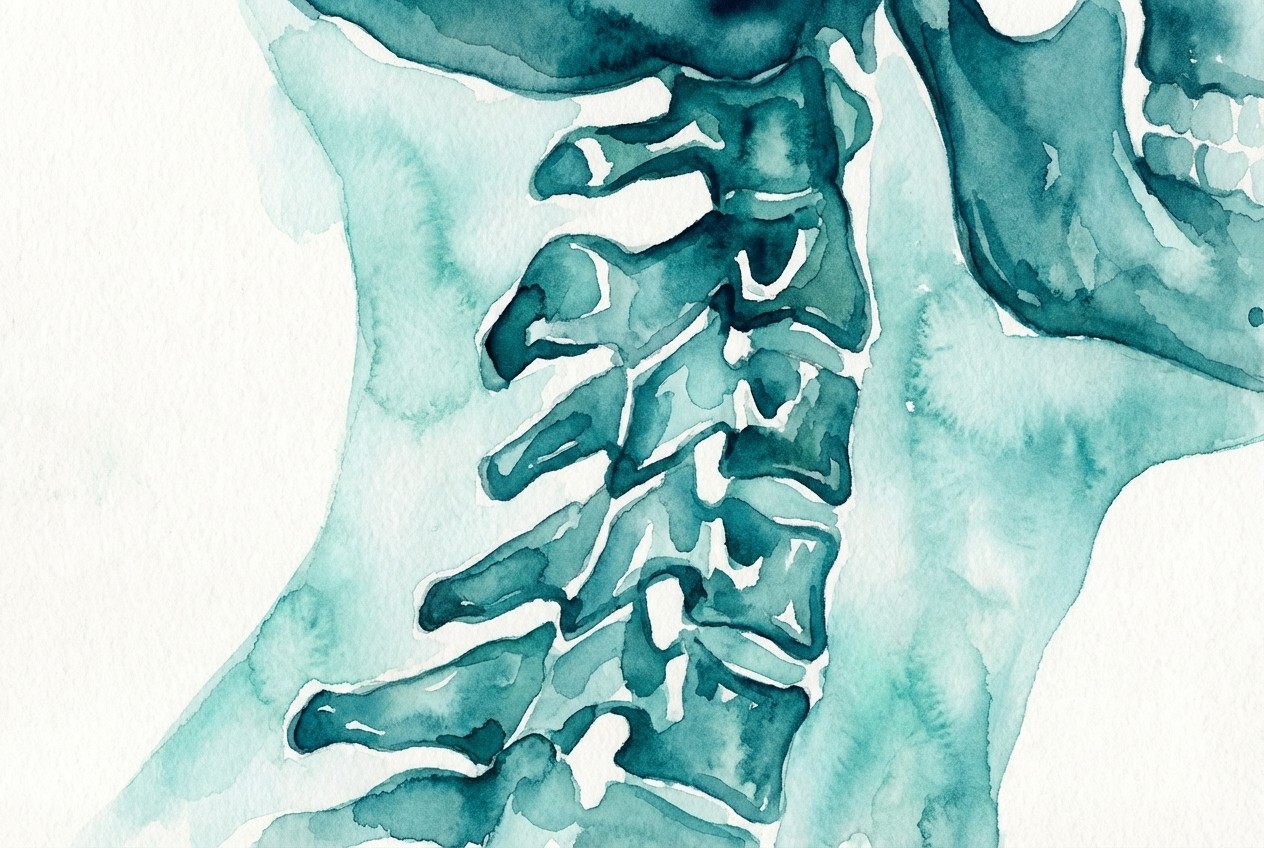
The ice pick. The pressure and throbbing episodes. The beam through my eye and the debilitating days that stole three quarters of every month. In my case, all of it traced back to Craniocervical Instability (CCI).
The ligaments at the top of my spine weren’t holding the joint in place. The instability was placing strain on everything around it. My body had been sending distress signals for years. Every description I gave my doctors had been accurate. They had the wrong diagnosis.
None of it appeared on my standard MRIs. A Digital Motion X-ray captured slippage between C1 and C2 when my head moved. Additional imaging confirmed the diagnosis of CCI.
I had spent years treating symptoms that all had the same source. I had come within one appointment of burning a nerve without anyone ever finding it.
What I Carry Forward
Nine months after surgery. My husband drove me and the girls to New York City for my follow-up appointment. Four and a half hours each way. The ice pick was there for most of it. So was the swallowing, the sensation of something caught in my throat, of being slowly strangled from inside. It comes back every time I’m in a car.
My neurosurgeon told me that for many patients with the tissue disorder, travel does that. The titanium holds the structure in place but the motion still finds a way in. He referred me to an ENT for the swallowing and back to a neurologist to revisit trigger point injections and an occipital nerve block.
We drove home with two new referrals.
If you’ve been through every specialist and still don’t have an answer, the answer may not be in the specialist. It may be in the test. Some problems need a different kind of imaging to see them.
Want to understand the structural cause?
Craniocervical Instability (CCI): A Patient’s Perspective.
Every stripe tells part of the story.
The full story begins in You Might Be a Zebra: Rare Unveiled.


Please note: This information is provided for general reference only and is not based on medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for medical concerns.